

Abstract
Background
Darwinian evolution drives multiple myeloma (MM) and leads to diversity both within and between patients. This suggests the need for combinations of agents with different mechanisms of action targeting sub-clonal populations to maximize the depth of response and improve outcomes. Approaches to maximize response pre-transplant include the use of sequential pre-transplant consolidation with a different agent in sub-optimal responders or intensifying upfront combinations whilst aiming to minimize additional toxicities.
Carfilzomib is a novel irreversible inhibitor of the proteasome that has been suggested to have greater activity than bortezomib, with deeper responses and improved outcomes. The Myeloma XI phase III randomized trial for newly diagnosed MM patients compared intensified induction with the quadruplet KCRD vs a response adapted approach of sequential triplet therapies for transplant-eligible MM patients.
Methods
KCRD was given in 28 day cycles (carfilzomib (K) 36mg/m2 IV d1-2, 8-9,15-16 (20mg/m2 #1d1-2), cyclophosphamide (C) 500mg PO d1,8, lenalidomide (R) 25mg PO d1-21, dexamethasone (D) 40mg PO d1-4,8-9,15-16), CRD in 28 day cycles (C 500mg PO d1,8, R 25mg PO d1-21, D 40mg PO d1-4, 12-15) or CTD in 21 day cycles (C 500mg PO d1,8,15 thalidomide (T) 100-200mg PO daily, D 40mg PO d1-4,12-15). All induction regimens were continued for a minimum of 4 cycles and to maximum response. Suboptimal responders (MR/PR) to CTD/CRD were randomized between pre-transplant intensification with a proteasome inhibitor (bortezomib, CVD) containing triplet or no further therapy prior to ASCT, patients with refractory disease (SD/PD) all received CVD. For all patients a maintenance randomization 3 months post ASCT compared lenalidomide given to disease progression to observation. Cytogenetic data, centrally analyzed, was available for a representative subset of patients. High-risk was classified as presence of t(4;14), t(14;16), t(14;20), del(17p) or gain(1q) and ultra-high risk the presence of more than one lesion.
1056 patients underwent induction randomization between December 2013 and April 2016 and were allocated to CTD n=265, CRD n=265, KCRD n=526. The groups were well matched across baseline variables with median age 61 (range 33-75). The median follow up for this analysis is 34.5 months. The independent data monitoring and ethics committee recommended immediate release of the data following an interim analysis.
Results
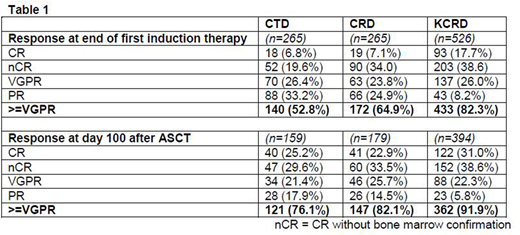
Intention to treat analysis of the initial induction regimens found that KCRD was associated with a significantly longer PFS than triplet therapy (HR 0.63, 95%CI 0.51, 0.76, median PFS KCRD NR vs CTD/CRD 36.2 months, p<0.0001). Improved PFS was seen in all cytogenetic risk groups. PFS2, a key secondary endpoint, was also significantly improved with KCRD (HR 0.75, 95% CI 0.56, 0.99, 3yr PFS2 KCRD 81.8% vs CTD/CRD 75.1%). Deeper response rates were seen in patients treated with KCRD vs CTD/CRD both pre and post transplant (p<0.0001), Table 1.
All regimens were well tolerated with no significant additional toxicity due to the quadruplet regimen. KCRD was administered for a median of 4 cycles, CRD 5 cycles and CTD 6 cycles. Grade 3+ neutropenia occurred in 16.4% KCRD, 22.3% CRD and 12.8% CTD patients and thrombocytopenia in 8.4% KCRD, 2.3% CRD and 1.2% CTD patients. A higher proportion of patients receiving KCRD induction were able to undergo ASCT than those who received response-adapted induction. In an analysis restricted to those who had completed ASCT, KCRD induction was still associated with a significantly longer PFS.
An exploratory analysis compared the patients receiving KCRD to patients in the CTD/CRD arm who had received the optimum response-adapted approach (i.e. excluding those randomized to no CVD following MR/PR). The quadruplet was associated with significantly longer PFS than using a response adapted sequential triplet approach (HR 0.64, 95% CI 0.52, 0.78, p<0.0001).
Conclusions
This large randomized study of a carfilzomib containing quadruplet combination, KCRD, demonstrates that it is well tolerated and associated with deep responses both pre- and post-transplant and has a significant PFS and PFS2 benefit compared to triplet therapy. The benefit of upfront intensification of treatment persisted even compared to triplets administered sequentially and including exposure to both lenalidomide and bortezomib.
On behalf of the NCRI Haem-oncology CSG
Jackson:Merck Sharp and Dohme: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau; Roche: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria, Other: Travel Support, Research Funding, Speakers Bureau; Takeda: Consultancy, Honoraria, Other: Travel Support, Research Funding, Speakers Bureau. Davies:Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees; Abbvie: Consultancy; ASH: Honoraria; MMRF: Honoraria; Janssen: Consultancy, Honoraria; TRM Oncology: Honoraria. Pawlyn:Janssen: Honoraria, Other: Travel support; Celgene Corporation: Consultancy, Honoraria, Other: Travel support; Amgen: Consultancy, Honoraria, Other: Travel Support; Takeda Oncology: Consultancy, Other: Travel support. Cairns:Merck Sharp and Dohme: Research Funding; Amgen: Research Funding; Celgene: Research Funding. Striha:Amgen: Research Funding; Abbvie: Research Funding; MSD: Research Funding; Celgene: Research Funding; Janssen: Research Funding. Hockaday:MSD: Research Funding; Janssen: Research Funding; Celgene: Research Funding; Amgen: Research Funding; Abbvie: Research Funding; Millenium: Research Funding. Collett:Amgen: Research Funding; Celgene: Research Funding; Merck Sharp and Dohme: Research Funding. Jones:Celgene: Honoraria, Other: Travel support, Research Funding. Kishore:Takeda: Honoraria, Other: travel support; Celgene: Honoraria. Garg:Novartis: Other: travel support, Research Funding; Amgen: Honoraria, Other: Travel Support; Janssen: Honoraria; Takeda: Other: Travel Grant. Williams:Amgen: Honoraria, Speakers Bureau; Novartis: Honoraria; Janssen: Honoraria, Other: travel support, Speakers Bureau; Takeda: Honoraria, Other: travel support, Speakers Bureau; Celgene: Honoraria, Other: travel support, Speakers Bureau. Karunanithi:Janssen: Other: Travel support, Research Funding; Celgene: Other: Travel support, Research Funding. Lindsay:Takeda: Other: Travel support; BMS: Consultancy, Other: Travel support; Janssen: Consultancy; Celgene: Honoraria, Other: Travel support; Novartis: Other: Travel support. Jenner:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Cook:Celgene Corporation: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Seattle Genetics: Honoraria; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Bristol-Myers Squibb: Consultancy, Honoraria; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau; Glycomimetics: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria, Speakers Bureau. Russell:Jazz Pharma: Speakers Bureau; Daiichi Sankyo: Consultancy; Pfizer: Consultancy, Honoraria, Speakers Bureau. Kaiser:Bristol-Myers Squibb: Consultancy, Other: travel support; Amgen: Consultancy, Honoraria; Takeda: Consultancy, Other: travel support; Janssen: Consultancy, Honoraria; Chugai: Consultancy; Celgene: Consultancy, Honoraria, Research Funding. Drayson:Abingdon Health: Equity Ownership, Membership on an entity's Board of Directors or advisory committees. Owen:Janssen: Consultancy, Other: Travel support; Celgene: Consultancy, Honoraria, Research Funding; Takeda: Honoraria, Other: Travel Support. Gregory:Celgene: Consultancy, Honoraria, Research Funding; Janssen: Honoraria; Amgen: Research Funding; Merck Sharp and Dohme: Research Funding. Morgan:Bristol-Myers Squibb: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Janssen: Research Funding; Celgene: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal